由臺灣燒傷暨傷口照護學會、台灣傷口照護學會、台灣傷口造口及失禁護理學會與德國慢性傷口協會(Initiative of Chronic Wound, ICW)、國際品質監督體系德國萊茵(TÜV Rheinland)合作之國際傷口師認證課程,即將於2025年4月18日假衛生福利部雙和醫院開課。
本培訓課程係由臺灣燒傷暨傷口照護學會、台灣傷口照護學會、台灣傷口造口及失禁護理學會、德國慢性傷口協會(ICW)和國際品質監督體系德國萊茵(TÜV Rheinland)共同舉辦,培訓合格的學員將獲得由主辦單位及ICW聯合頒發,TÜV認證的國際傷口治療師證書。培訓課程獲歐洲傷口協會(EWMA)認可,與美國傷口管理協會(AWMA)的認證培訓等同,被認為當今國際最高水準的傷口管理培訓課程之一。歡迎有意參加者,踴躍報名。
一、主辦單位:臺灣燒傷暨傷口照護學會、台灣傷口照護學會、台灣傷口造口及失禁護理學會、中山醫學大學附設醫院整形外科
二、協辦單位:社團法人台灣在宅醫療學會、社團法人台灣居家護理暨服務協會
三、贊助單位:台灣赫曼有限公司
四、培訓目的:因應高齡化社會與長者照護之需求,培養具有國際視野的從事傷口治療與護理的高級傷口治療專業人才,提高其對現代傷口治療理論及各類傷口的評估、處理、評價等技巧的認知及運用能力,具備獨立處理各類疑難傷口的能力,並能帶動、提高和指導臨床醫務工作者傷口治療的整體水準。培訓國內具國際認證之傷口照護人員,以提升慢性傷口照護品質。
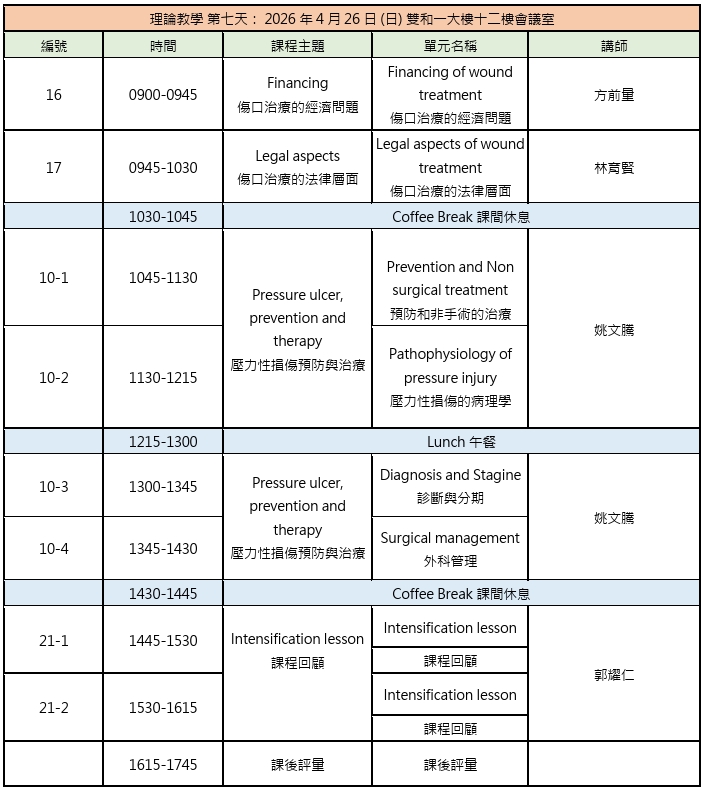
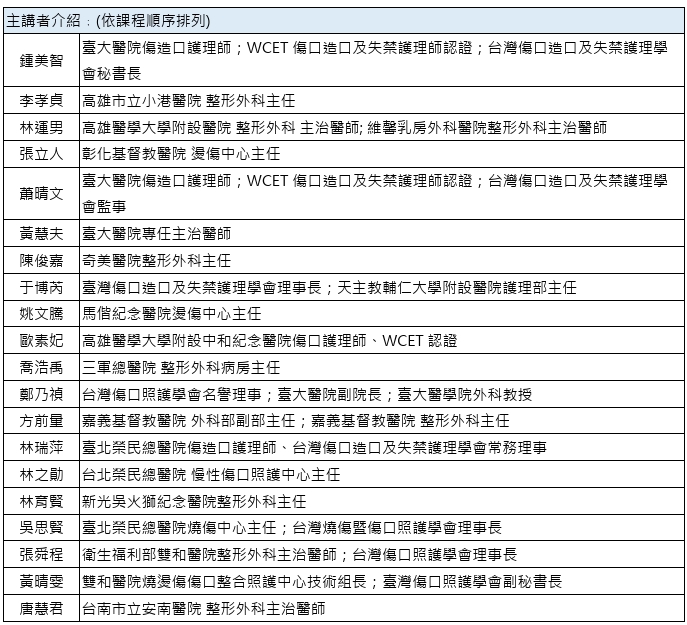
五、課程內容及師資:培訓的課程設置分為理論教學和臨床實習兩部分。授課師資將由國內知名專家組成,主辦單位將邀請具有豐富培訓經驗的講師以及臨床醫療、護理專家授課。
※本課程教材為英文編寫 (搭配中文關鍵字),中文授課。
六、報名資格條件:具合格證照之護理師(士)、專科護理師或臨床醫療從業人員。
(一)工作上有照護慢性傷口需求之醫療人員。
(二)臨床經驗1年以上內外科臨床護理經驗者。
七、訓練期程:需完成56堂的面授課程以及16小時的實習課程。
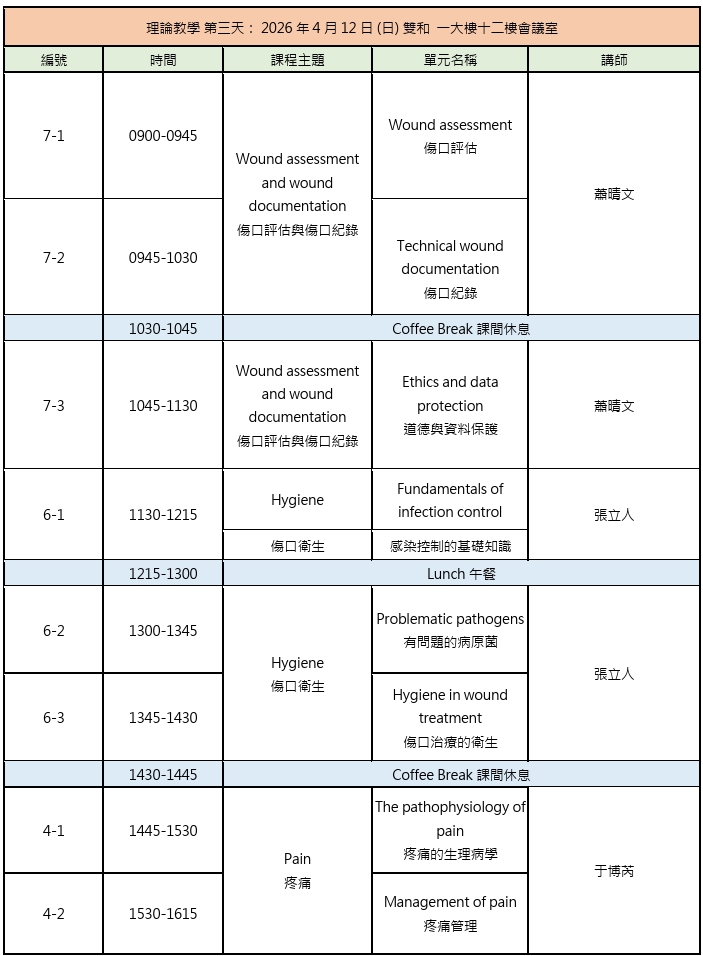
(一)理論教學:
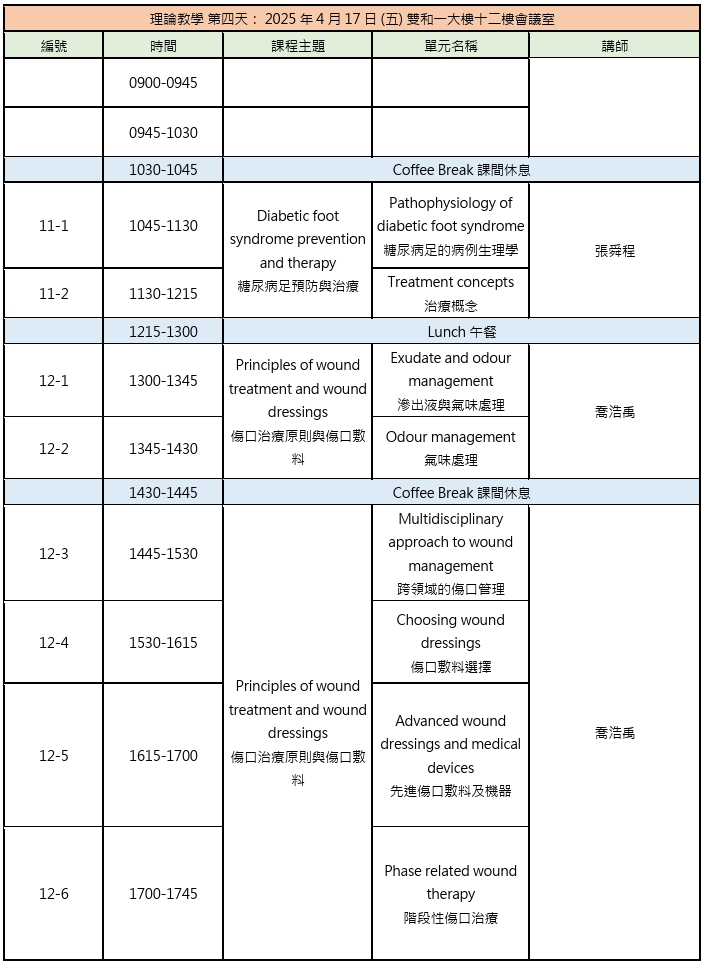
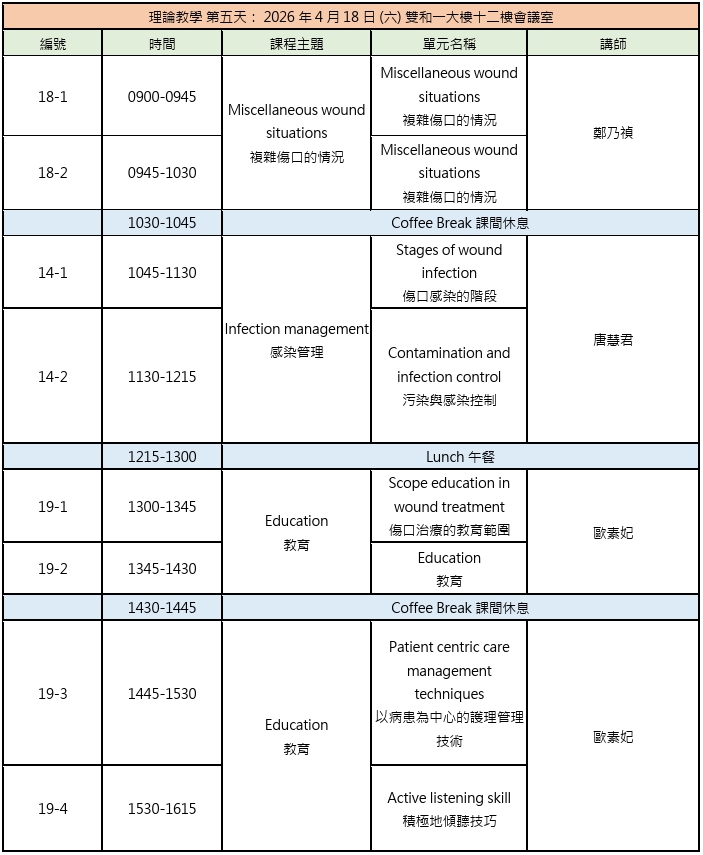
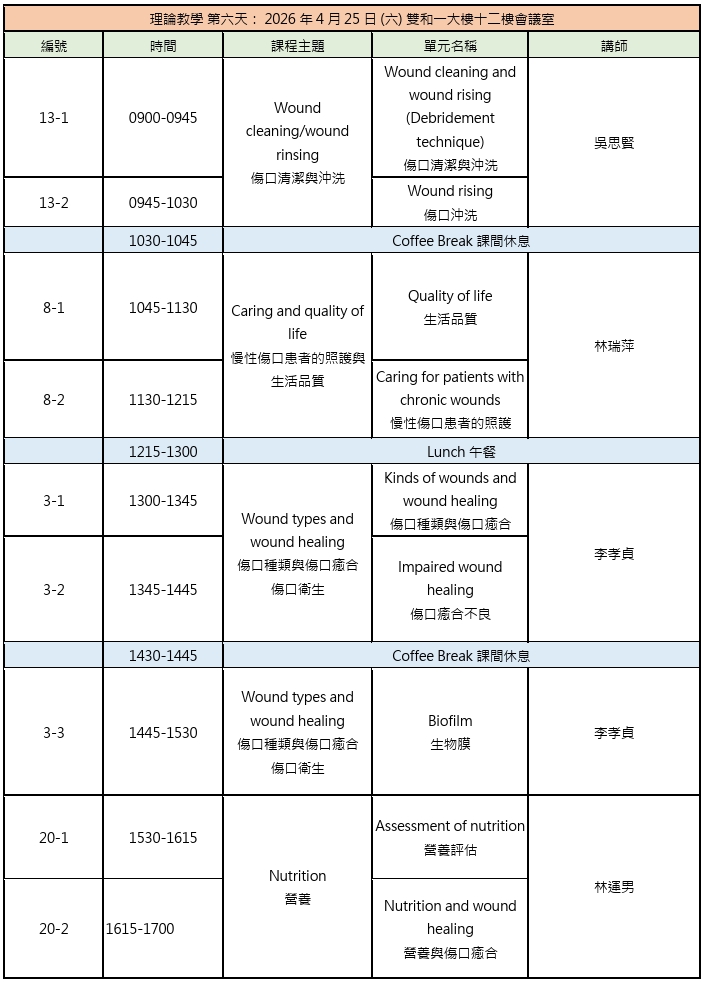
2026年4月10日(五)、4月11日(六)、4月12日(日)、4月17日(五)、4月18日(六)、4月25日(六)、4月26日(日),計7日。
(二)臨床實習:
2026年5月7日(四)、5月15日(五),計2天,會依見習醫院的醫師時間做調整。
八、上課地點
(一)理論教學:衛生福利部雙和醫院一大樓12樓會議室 (235新北市中和區中正路291號)。
(二)臨床實習:臺大醫院、台北榮總、新光醫院、馬偕醫院、三軍總醫院、林口長庚、衛生福利部雙和醫院;由主辦單位安排。
九、報名時間:即日起至2026年3月20日前額滿為止。
十、招生名額:正取25名,備取2名。主辦單位可依報名學員之臨床實務年資、傷口處置相關經驗決定正取名單。
十一、報名方式:本次課程採線上報名審查,點此連結
(https://forms.office.com/e/SvJY6RgKs3?origin=lprLink)線上報名,並請於線上報名後3日內(含報名當日)mail報名資格證明附件至[email protected],並於主旨註明「報名國際傷口師認證課程-報名資格證明附件」
※報名資格證明附件為:
1. 合格有效之護理師、專科護理師或醫師證書(請提供PDF掃描檔)
2. 合格有效之學位證明
※其他有利審查之附件:
1. 曾發表傷口相關之論文或海報 2. 工作單位主管推薦信 3. 參與主辦學會舉辦活動證明(如課程,年會,研討會)
※其他有利審查之經驗:
1. 參與工作單位的傷口護理 2. 能決定工作單位的傷口護理策略 3.每個月慢性傷口個案數 (DMF/PI/LU) 4. 臨床上處理的遭遇的傷口種類
※線上報名後,請儘速將報名資格證明附件mail至協辦單位信箱([email protected]),以利主辦單位辦理行政審核,結果將陸續於主辦學會網站公告錄取名單並通知錄取當事人,通知錄取後請於一個星期內完成繳費匯款,始完成報名程序。逾時未完成繳費,名額將由備取學員遞補。
十二、報名費用:每人新臺幣$45,000元整,費用含餐點、講義,不含個人上課及實習期間住宿與往返交通費。確認錄取後,將另行寄出繳款單,請於期限內繳款,以完成報名手續。
十三、評分方式及取得證書:
(一)學員按培養計畫順利完成全部課程及臨床實習,通過專業理論考核─23題中文問答題和案例書面報告後,可獲得由臺灣燒傷暨傷口照護學會、台灣傷口照護學會、台灣傷口造口及失禁護理學會、ICW頒發、TÜV、EWMA認證的國際傷口治療師證書,證書有效期5年,期滿且修滿ICW認可的繼續教育學分(每年需要8學分,5年共40學分) 後可更新。
(二)若專業理論考核和案例書面報告有未通過者,有兩次補考機會,補考時將酌收費用NT$1,000元/次。
十四、如有疑問請洽台灣赫曼,陳小姐。
電話:(02)2790-7992分機12
E-mail:[email protected]
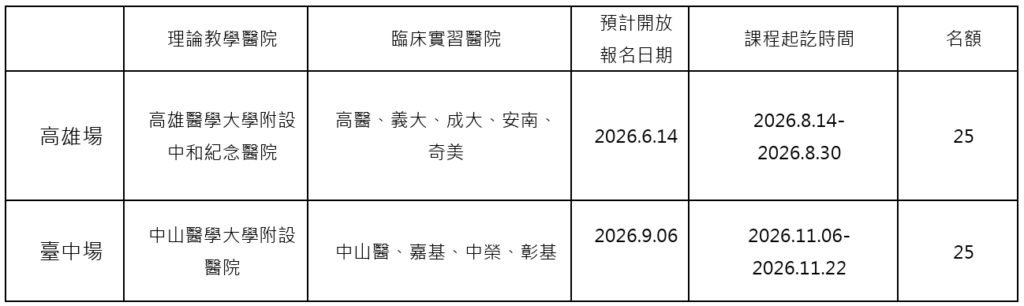
十五、其他梯次課程預告:
十六、課程表:慢性傷口基礎照護課程

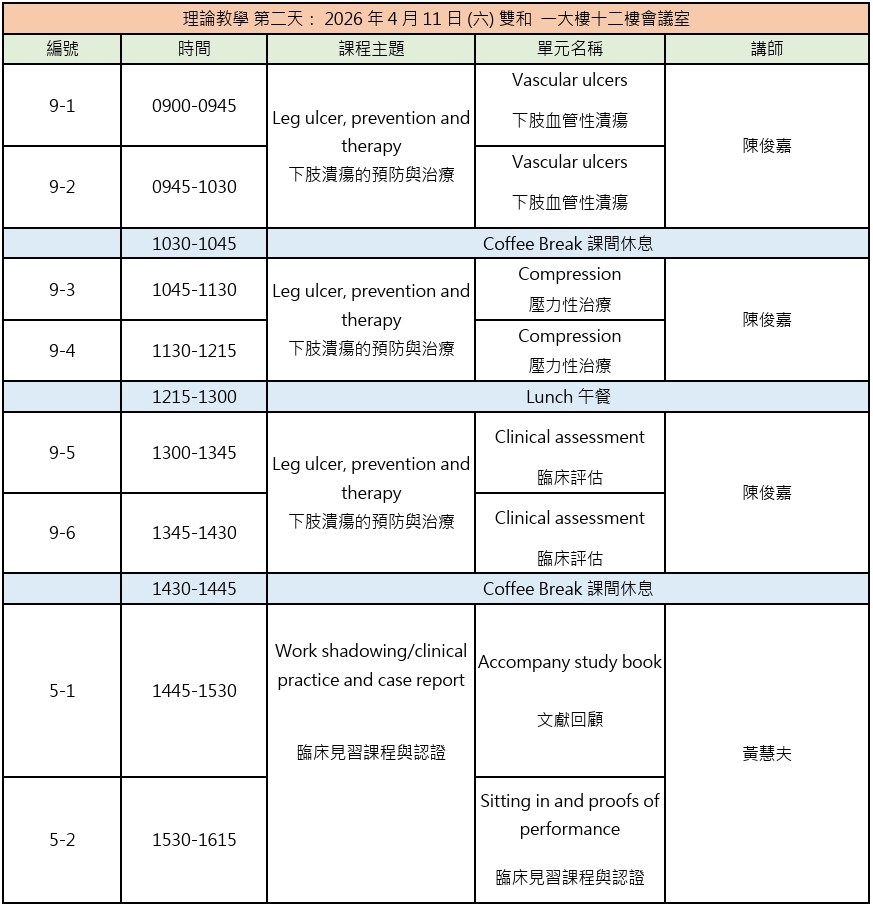
※課程上課時間主辦單位保留更改的權利,若有更改會立即於學會網站更正。
")